
Round Zero: an initiative for the early screening of Combat Sport Athletes to improve mental health outcomes
Rhiana Roque M.D., Psychiatrist/Sports Psychiatrist November 2025
GOAL
To create an effective and efficient mental health screening process for combat sports athletes, that can easily be applied to various typical combat sports settings.
PURPOSE
To identify mental health symptoms as early as possible, to support optimization of sport performance, overall athlete well-being, and provide medical or psychosocial interventions when necessary.
TOOL
International Olympic Committee’s validated screening tool Sport Mental Health Assessment Tool 1 (SMHAT-1).
Introduction
It is well-known that exercise and sport participation can be beneficial to mental health. Equally true however, is the fact that athletes have unique challenges and factors that pose a risk to their mental wellbeing. These include injury and overtraining, pressure to perform at peak levels, maladaptive perfectionism, intense public scrutiny particularly in this age of social media, stigma associated with seeking help, and organizational and systemic stressors. Combat sports athletes are no different, and if anything have additional risk factors including higher incidence of sport-related concussions, regularly having to cut weight, the lack of a clearly defined and predictable season, and the possibility fight cancellations leading to loss of income and demoralization.
These contribute to both short-term and lasting psychological and neuropsychiatric symptoms including depression, anxiety, addictions, and disordered eating. Research suggests that current elite athletes experience comparable or slightly higher rates of anxiety and depression (34%), alcohol misuse (19%), and sleep disturbances (26%).[1] The International Olympic Committee (IOC) consensus statement on mental health in elite sports reports that anxiety and depression can occur in up to 45% of elite male athletes in team sports.[2]
In the context of sport and the even broader context of life, optimal mental health is a core component of well-being. Drawing on the consensus statement created by an international Think Tank in 2020, mental health is a valuable resource for athletes to draw from through their entire careers – in periods of stress, transitions, and decision-making. The sports environment and culture should be seen as having the potential to nourish or malnourish the mental health of an athlete.[3]
This brief paper outlines how a mental health screening tool developed by the IOC can be adapted and applied to benefit combat sports athletes.
The Sports Mental Health Assessment Tool in a nutshell:
WHAT
The SMHAT-1 is a seminal screening tool developed in 2020 by the IOC Mental Health Working Group of 11 international experts to identify elite athletes who are at increased risk for or already have mental health symptoms and disorders.[4]
WHO
The first two steps are self-administered by athletes, but the responses must be promptly reviewed and scored by a qualified member of the team. If the scores are sufficiently high, the subsequent components are to be administered by a health professional or sports medicine physician.
WHEN
The IOC recommends administering this three times a year (pre-season, mid-season, and end-season). It is also recommended to be administered when any significant event occurs such as injury, concussion, illness, surgery, unexplained performance concerns, suspension from play, suspected harassment or abuse, and adverse life events or transitions.
However, due to the absence of seasons in combat sports, this can be given as part of the entrance physical exam. It is this writer’s recommendation that it be given thereafter as part of an annual physical exam, and at least every six months thereafter.
WHERE
No special examination room or equipment is required. The portions to be completed by a health professional or physician are ideally administered in person but can also be done remotely (via telehealth).
*** Athletes responses must be reviewed and scored promptly (this writer recommends within 24 hours), in order to swiftly intervene and refer urgently/emergently the athlete who has thoughts of suicide or self-harm. ***
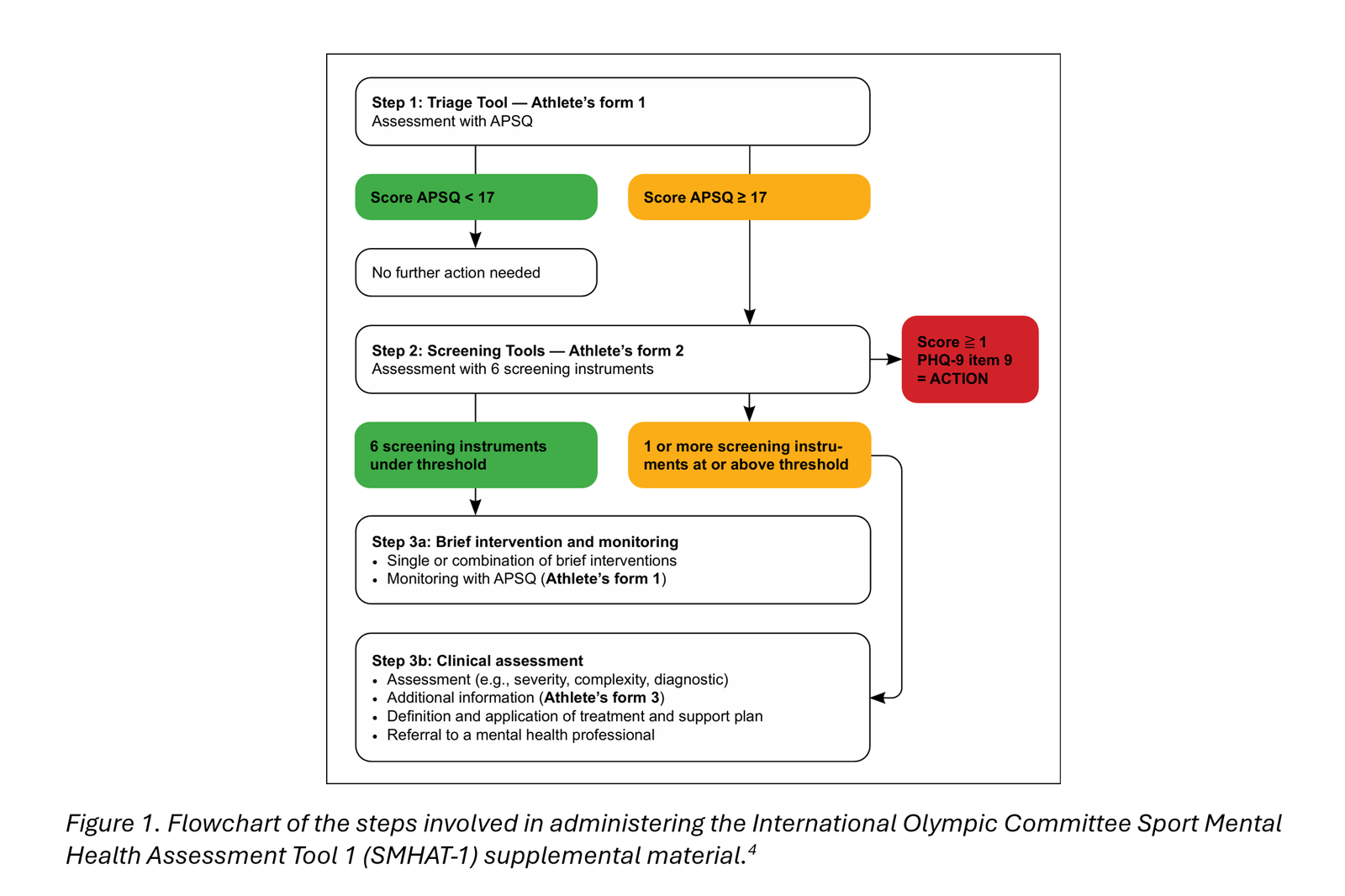
Components of the SMHAT-1:
Step 1 – Basic Triage
The athlete completes the Athlete’s Form 1, comprised of 10 questions related to the frequency of mental health symptoms occurring in the past 30 days related to anxiety, depression, cognitive and behavioral manifestations, and functional impairment.
If an athlete scores 16 or below, no further action is needed. A score of 17 or above, the athlete moves on to Step 2.
*** Caveat – two follow-up studies on the SMHAT-1 in Team USA athletes note a high false negative rate of the Athlete’s Form 1. [5,6] The first study suggests it may be better that Step 1 and 2 be combined and administered together. The alternative is to add the question asking about suicidal and self-harm thoughts from Athlete Form 2, at the very least, in order not to miss risk of self-harm. However, the IOC has not yet formally updated the SMHAT-1 to incorporate this new finding. ***
Step 2 – Expanded Screening
If the athlete has a score of 17 and above, they then complete the Athlete’s Form 2. This consists of established and clinically validated instruments utilized in mental health, across six domains. Specifically, these questionnaires are:
- General Anxiety Disorder-7 (GAD-7) for general anxiety
- Patient Health Questionnaire-9 (PHQ-9) for depressive symptoms and thoughts of suicide or self-harm
- Athlete Sleep Screening Questionnaire (ASSQ) to identify sleep problems
- Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) to identify at-risk drinking
- Cutting Down, Annoyance by Criticism, Guilty Feeling, and Eye-openers Adapted to Include Drugs (CAGE-AID) to screen for substance abuse issues
- Brief Eating Disorder in Athletes Questionnaire (BEDA-Q) to identify disordered eating symptoms. Note that the last three questions may need to be modified in the combat sport population to exclude event-related weight-cutting
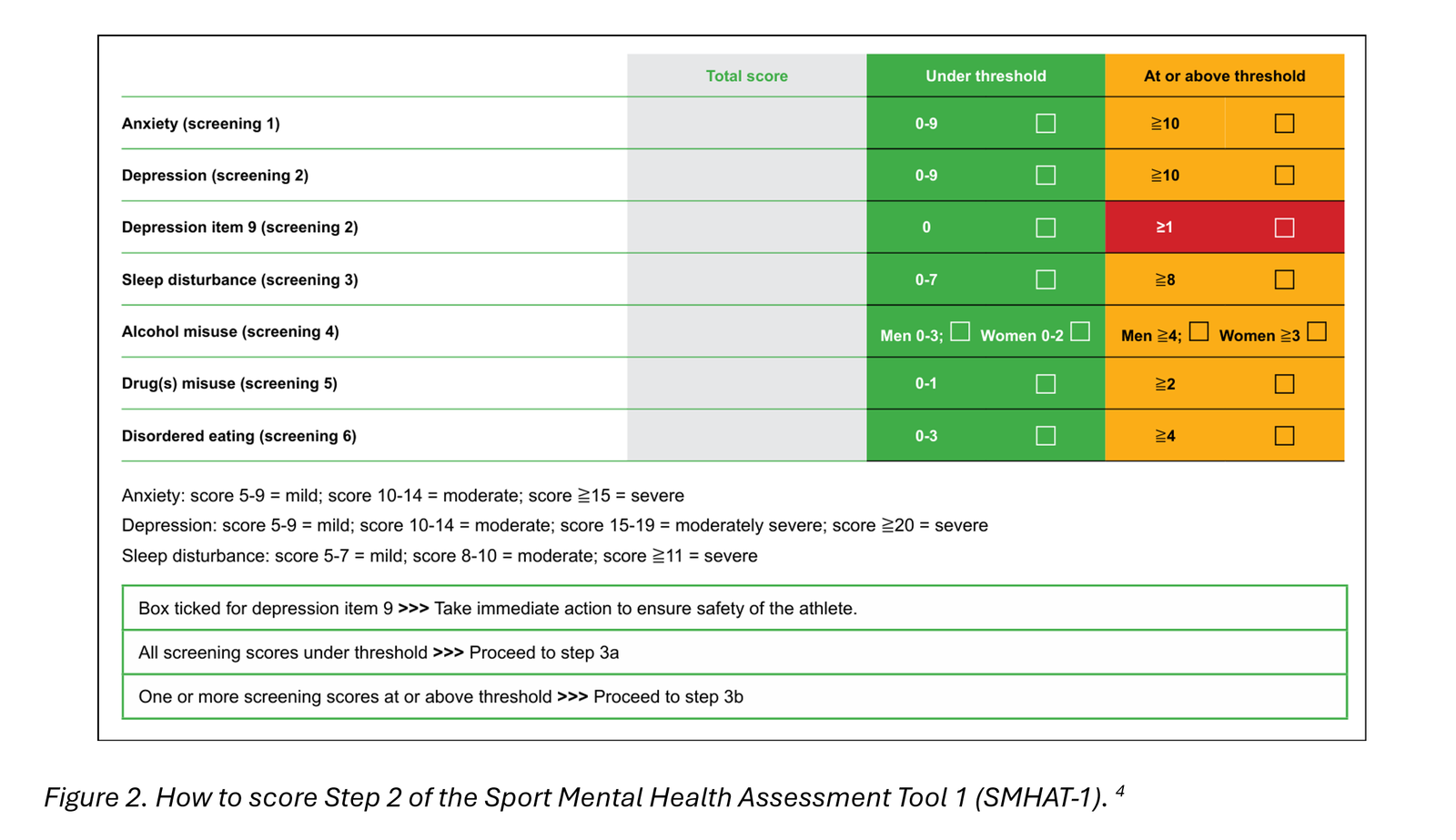
A member of the team reviews and scores the responses. Each questionnaire has its own cutoff scores. If the athlete does not meet the cutoff score for any of the questionnaires, they move forward to Step 3a (see below). If the athlete is above the cutoff score for any of the questionnaires, they move on to Step 3b.
*** If the athlete answers positive to the specific question regarding having suicidal or self-harm thoughts (question 9 in the PHQ-9), an immediate referral for Urgent or Emergent Evaluation is required to ensure the safety of the athlete. ***
Step 3a – Brief Intervention and Monitoring for milder cases
This is for the athlete who scored above the cutoff in Step 1 but below the cutoff in Step 2, suggesting only mild difficulties and impairment within the past month. Management consists of at least one brief intervention that provides additional knowledge and tools for the athlete.
The following are examples of these brief interventions, provided over one or multiple sessions depending on the need:
- Psychoeducation on specific areas the athlete is shown to struggle with
- Mindfulness strategies
- Meditation and breathwork practice
- Mental skills training and stress management strategies
- Sleep hygiene and sleep management strategies
- Motivational interviewing for alcohol and substance use concerns
*** The IOC does not make a specific recommendation as to who should conduct the above, only that “the administrator might refer the athlete” to one receive the intervention(s). It is this writer’s opinion that the above be provided by a qualified mental health professional within the organization’s current ecosystem who is already involved in overseeing the project. ***
After the intervention(s), the athlete will be reassessed using Athlete’s Form 1 (back to Step 1). If positive (score of 17 or greater), the athlete bypasses Step 2 and proceeds to Step 3b.
Step 3b – Clinical Assessment and Management for moderate cases and above
This is for the athlete who scores above the cutoff in any of the 6 expanded screening instruments in Step 2, suggesting symptom severity and functional impairment is of at least a moderate degree. It is also for the athlete who went through Step 3a but scored positive again in the Athlete Form 1 after the brief intervention, suggesting lack of response. It is likely that an athlete in this category will meet diagnostic criteria for a diagnosable mental health disorder(s).
Clinical Assessment
The IOC recommendation is for this part to be completed by either a licensed/registered mental health professional or a sports medicine physician.[4]
*** It is this writer’s opinion that it would be ideal for a sports medicine physician (psychiatrist or non-psychiatrist) to conduct this step, as it involves a comprehensive clinical assessment of a higher complexity, taking into account the medical and sports contexts, with the goal of creating an individualized management plan. ***
The clinician needs to consider the severity, complexity, and diagnostic uncertainties involved such as comorbid medical or mental health conditions or diagnoses, and sport and non-sport issues. These can include the existence of Attention Deficit Hyperactivity Disorder (ADHD), Relative Energy Deficiency in Sports (RED-S), diabetes, recent injury, history of childhood trauma, unhealthy coping strategies, financial stress, or recent suspension from play.
If additional information may be helpful, the clinician can administer Athlete’s Form 3, comprised of validated screening instruments in five additional domains:
7. Adult ADHD Self-Report Scale (ASRS) to screen for Attention Deficit Hyperactivity Disorder
8. Mood Disorder Questionnaire (MDQ) to assess the likelihood of Bipolar Disorder
9. Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) to screen for Post Traumatic Stress Disorder
10. Problem Gambling Severity Index (PGSI) to identify problem gambling and Gambling Disorder
11. Prodromal Questionnaire-16 (PQ-16) to screen for prodromal Psychotic Disorder
The dangerousness and urgency of the current clinical problem must also be determined. For example, factors such as suicidal or homicidal thoughts, electrolyte abnormalities in the presence of an eating disorder, paranoid delusions, or command hallucinations must be evaluated.
Clinical Management
The appropriate individualized management plan must then be formulated. The athlete’s response to treatment must be monitored regularly and the plan reformulated as necessary.
In cases that are neither severe, complex, nor diagnostically uncertain, the IOC notes that treatment and support can be provided by a sports medicine or primary care physician, provided they feel competent and comfortable in doing so. For guidance, they can refer specifically to the other seminal publication, the IOC Consensus Statement on Mental Health in Elite Athletes.[2,4]
Treatments and interventions that can be provided by a clinician at this level can include:
- Managing insomnia with a sleeping aid like melatonin or Trazodone
- Screening for sleep apnea
- Prescribing an antidepressant
- Management of a mild case of RED-S
- Referral to a dietitian
- Differentiating between Functional Overreaching vs. Overtraining Syndrome
- Evaluating concussions and return to play
In cases that are severe, complex, diagnostically uncertain, and/or non-responsive to the management that has been provided, further referral/s to a licensed mental health professional (sports psychiatrist or sports psychologist) for psychotherapy and medication management, and programs (e.g., substance use program, eating disorder program) are warranted.
Conclusion
While athlete mental health is meant to be “everybody’s business,” the time has come for sports organizations to finally do something about it being “nobody’s responsibility.”[3] A systematic screening strategy assigned to one or a few specified members is the long-overdue first step.
Combat sports organizations owe it to their athletes to finally prioritize, invest in, and create the infrastructure to promote the early identification and management of mental health symptoms to help athletes succeed and thrive, because true winning for everyone starts before the first bell.
References:
1. Gouttebarge V, Castaldelli-Maia JM, et al. Occurrence of mental health symptoms and disorders in current and former elite athletes: a systematic review and meta-analysis. British Journal of Sports Medicine. 2019;53:700-707.
2. Reardon CL, Hainline B, Aron CM, et al. Mental health in elite athletes: International Olympic Committee consensus statement (2019). British Journal of Sports Medicine. 2019;53:667–699.
3. Henriksen K, Schinke R, et al. Consensus statement on improving the mental health of high performance athletes. International Journal of Sport and Exercise Psychology. 2020;18:5:553-560.
4. Gouttebarge V, Bindra A, Blauwet C, et al. International Olympic Committee (IOC) Sport Mental Health Assessment Tool 1 (SMHAT-1) and Sport Mental Health Recognition Tool 1 (SMHRT-1): towards better support of athletes’ mental health. British Journal of Sports Medicine. 2019;0:1-9 and supplemental material.
5. Anderson T, Adams WM, Bartley JD, et al. Analysis of the Sport Mental Health Assessment Tool 1 (SMHAT- 1) in Team USA athletes. British Journal of Sports Medicine. 2023;57:1187–1194.
6. Anderson T, Bartley A, et al. Update on sport mental health assessment tool- 1 false negative rates from the 2024 Paris Olympic and Paralympic Games. BMJ Open Sport & Exercise Medicine. 2025;11:e002608.
Additional Resources:
Disclaimer – the information on this website does not constitute medical advice. No doctor-patient relationship is formed. Please seek the attention of a qualified medical professional for your concerns.
Expert Psychiatric Services tailored for athletes and those with active lifestyles, serving California and Nevada.
NEWS
Stay up to date on news and blog posts by subscribing to the ESMH newsletter below: